
One of the challenges for medical device manufacturers under the EU MDR is maintaining a coherent, timely update cycle across key technical documentation, particularly the Clinical Evaluation Report (CER), Post-Market Clinical Follow-up (PMCF), Periodic Safety Update Report (PSUR)/Post Market Surveillance Report (PMSR), and the Summary of Safety and Clinical Performance (SSCP) where required.
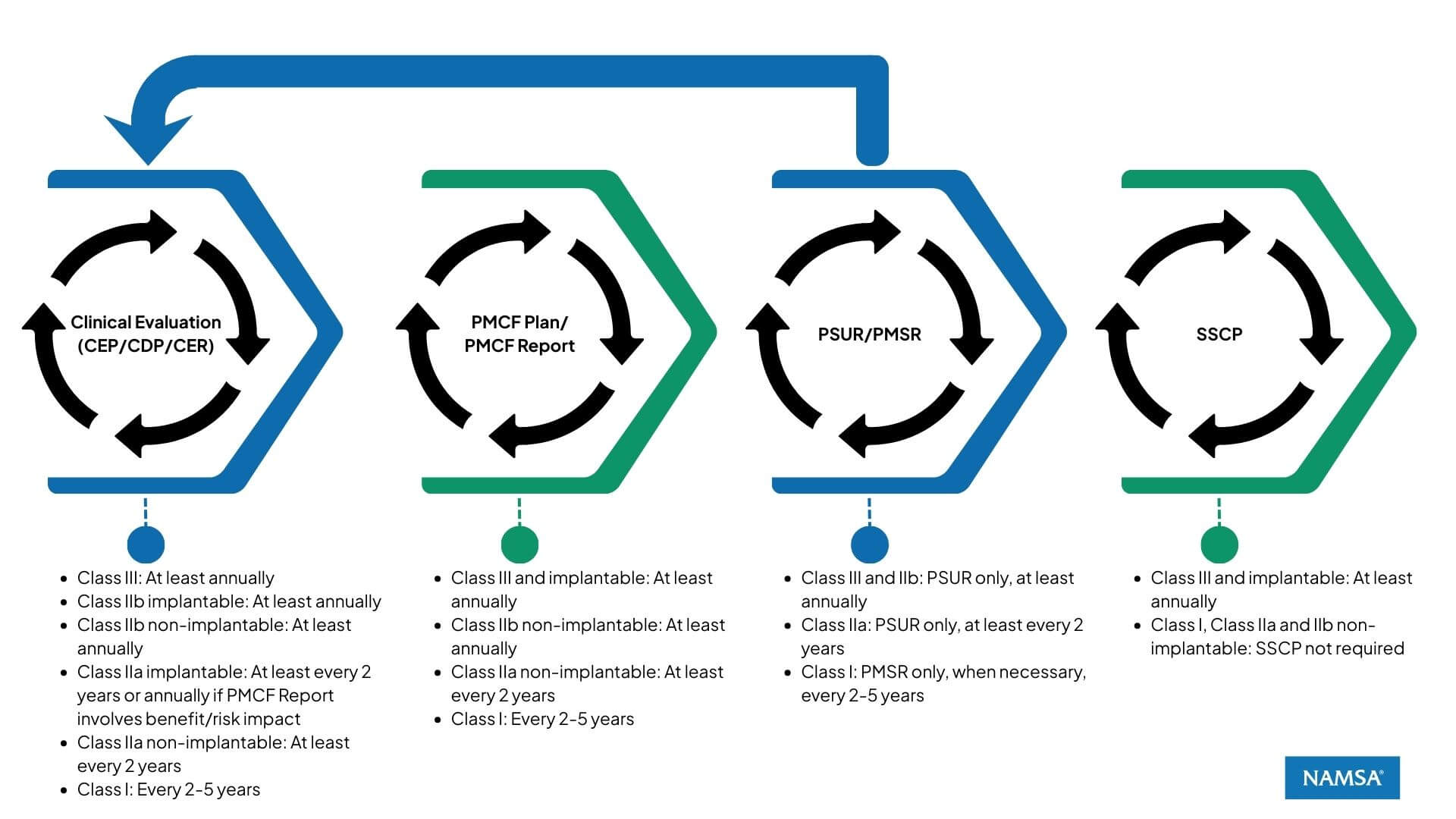
The MDR embeds these components in a dynamic feedback loop (Figure 1). Each document feeds into or depends on others, particularly based on the device’s risk classification and whether it is implantable.
Figure 1. The continuum loop of clinical evidence updates
CER – Clinical Evaluation Report
Update frequency (Linked to MDR Art. 61.11 & Art. 86.1):
It is important to note that CER update frequency is not described in the MDR, but the clinical evaluation is expected to be updated with the PMCF Report and PSUR/PMSR outputs. Then an indirect link is established with MDR Art.61.11, mentioning the annual update of the PMCF Report for the Class III and implantable devices (as well as the SSCP). MDR Art.86.1 describes the update frequency of the PSUR according to the classification of the device.
CER update requirements:
- Class III (implantable or not) & IIb implantable devices: At least annually, based on annually updated PMCF Report and PSUR
- Class IIb non-implantable device: At least annually, based on annually updated PSUR
- Class IIa implantable device: At least every 2 years, based on PSUR, or annually if the annually updated PMCF Report involves a benefit/risk impact
- Class IIa non-implantable: At least every 2 years, based on PSUR
- Class I: Every 2–5 years, according to MEDDEV 2.7/1 Rev. 4 section 6.2.3, or when the manufacturer receives new information from the PMSR that has the potential to change the current evaluation
- Custom-made devices: Not applicable
The CER, based on the Clinical Evaluation Plan (CEP), integrates clinical evidence from PMCF activities and safety signals from the PMSR/PSUR, ensuring clinical benefit/risk remains favorable over time.
The phrase “at least” in the context of the MDR update frequency (e.g., “at least annually”) sets a minimum requirement, not a fixed interval. This means that while updates must occur no less frequently than the stated period (e.g., annually for Class III and IIb implantable devices), earlier updates are expected if new information arises that could impact the device’s safety, performance, and/or benefit-risk profile. Such information may stem from PMCF activities, vigilance reports, PSUR findings, or other post-market surveillance data. Therefore, manufacturers must maintain a proactive and responsive clinical evaluation process, ensuring that the CER is updated as soon as necessary to reflect any significant changes in clinical evidence or risk assessment, in alignment with MDR Articles 61.11 and 86.1.
PMCF Plan/PMCF Report (Annex XIV Part B)
Update frequency (MDR Art. 61.11 & linked to MDR Art. 86.1):
Only the PMCF Report frequency of Class III and implantable devices is mentioned in the MDR Art. 61.11 (at least annually). For the other devices, it makes sense to align with the PSUR frequency (or for Class I devices the PMSR frequency).
- Class III & implantable devices (incl. custom-made): At least annually (MDR Art. 61.11)
- Class IIb non-implantable (incl. custom-made): At least annually, based on PSUR (Art. 86.1)
- Class IIa non-implantable (incl. custom-made): At least every 2 years, based on PSUR (Art.86.1).
- Class I (incl. custom-made): Every 2 to 5 years, based on CER cycle (per MEDDEV 2.7/1 revision 4 section 6.2.3 guidance), or when necessary, according to PMSR
This is a cornerstone of the CER update. A robust PMCF plan and report help detect clinical performance shifts early and support proactive risk management.
PSUR/PMSR
Update frequency (MDR Art. 85 & Art. 86.1):
- Class III and IIb (including custom-made): PSUR only, at least annually
- Class IIa (including custom-made): PSUR only, at least every 2 years
- Class I (including custom-made): PMSR only, at least every 2-5 years (based on per MEDDEV 2.7/1 revision 4)
The PMSR/PSUR synthesizes post-market data and acts as an early-warning tool for risk trends, which may trigger earlier CER updates or SSCP revisions where applicable.
Note: Sometimes during MDR submission, some manufacturers of Class IIa and above have submitted both PMSR and PSUR in their technical documentation. PMSRs are only required for Class I devices, all higher classifications only require a PSUR.
SSCP – Summary of Safety and Clinical Performance
Update frequency (MDR Art. 32 and Art. 61.11):
- Class III and implantable devices: At least annually
- Class IIa and IIb non-implantable: SSCP not required
- Class I and custom-made: SSCP not required
The SSCP is the public-facing document that reflects your device’s safety and performance claims. It must stay aligned with the most current version of the CER and PMCF data.
Note: If no changes or events impacting the safety, performance, or benefit-risk ratio occurred within the year, the SSCP could have the same content.
Final Notes on Custom-Made Devices
Custom-made devices fall outside of many standard obligations:
- No CER required
- No SSCP required
However, PMCF activities may still be relevant if risks are not well characterized or in case of incident trends:
- PMCF required (per MDR Annex XIII)
- PMSR or PSUR required (per MDR Art.85,86)
Conclusion: A Continuum Evidence System
Under MDR, the CER is not an isolated report. It is the central hub in a continuum system of clinical evidence. Manufacturers must ensure that:
- The PMCF plan/report feeds into the CER
- The PMSR/PSUR confirms safety signals and triggers updates
- The SSCP outputs align with the latest CER conclusions
Table 1 provides a summary of the update frequency per documentation and per classification of the subject device. Table 2 provides an example of implementation for a Class III legacy device.
Only by synchronizing these documents and respecting their update frequencies based on classification and implantability can you ensure compliance and clinical accountability under EU MDR.
Table 1. Update Frequencies: CER, PMCF Plan / Report, PSUR and SSCP
| Device Class/Type | CEP/CDP/CER | PMCF Plan / Report | PMSR / PSUR | SSCP |
|---|---|---|---|---|
| Class III (implantable or not) | At least annually | At least annually | PSUR at least annually | At least annually |
| Class IIb Implantable | At least annually | At least annually | PSUR at least annually | At least annually |
| Class IIb Non-implantable | At least annually | At least annually | PSUR at least annually | Not applicable |
| Class IIa Implantable | At least every 2 years, or annually if the PMCF Report involves a benefit/risk impact | At least annually | PSUR at least every 2 years | At least annually |
| Class IIa Non-implantable | At least every 2 years, aligned with PSUR/PMCF Report | At least every 2 years, aligned with PSUR | PSUR at least every 2 years | Not applicable |
| Class I (non-implantable) | Every 2–5 years, aligned with PMSR/PMCF Report | Every 2–5 years, aligned with PMSR | PMSR at least every 2–5 years | Not applicable |
| Custom-made | Not applicable | See above according to the classification | See above according to the classification | Not applicable |
Table 2. Case example: Class III legacy device cycle
| MONTH | CE CYCLE | 1/ PMS CYCLE => | 2/ PMCF CYCLE => | 3/ CER CYCLE => | 4/ SSCP CYCLE |
| YEAR 1 | |||||
| January | FIRST ISSUE after MDR TECH. DOC. SUBMISSION (First MDR CEP/CDP/CER, First PMCF PLAN/REPORT, First PSUR, First SSCP) | START DATA COLLECTION | START DATA COLLECTION | START DATA COLLECTION | START CYCLE |
| February | |||||
| March | |||||
| April | |||||
| May | |||||
| June | |||||
| July | |||||
| August | |||||
| September | |||||
| October | |||||
| November | |||||
| December | DATA LOCK | DATA LOCK | DATA LOCK | ||
| YEAR 2 | |||||
| January | DATA ANALYSIS | DATA ANALYSIS | LIT. SEARCHES/SOTA* | ||
| February | 2nd PSUR PREP. | 2nd PMCF REPORT PREP. | 2nd CEP.PREP | ||
| March | 2nd PSUR ISSUED=> | 2nd PMCF REPORT ISSUED=> | 2nd CEP ISSUED 2nd CER PREP. | ||
| April | 2nd CER ISSUED=> | 2nd SSCP PREP. | |||
| May | 2nd PMCF PLAN PREP. <= | 2nd SSCP ISSUED | |||
| June | |||||
| July | |||||
| August | |||||
| September | |||||
| October | |||||
| November | |||||
| December | DATA LOCK | DATA LOCK | DATA LOCK | DATA LOCK | |
*SOTA is the acronym for State-Of-The-Art, here referring to the clinical SOTA in the CER.
Frequently Asked Questions (FAQs)
Is it mandatory to update the CER annually for all devices?
No. Only Class III and implantable Class IIb devices require at least annual CER updates. Other classes follow the frequency of the underlying documents (PMCF and PSUR). For instance, Class IIa non-implantables may have their CER updated every two years, unless PMCF reveals significant changes.
What triggers an unscheduled update of the CER?
Any significant new clinical data (e.g., safety signals, emerging risks, updated PMCF findings, or changes in benefit/risk balance) may trigger an earlier CER update, even if the formal frequency hasn’t been reached.
Should PMCF always be performed, even for low-risk devices?
While PMCF may be less extensive for low-risk devices, it is still required unless justified otherwise, at least for the general activities (e.g. literature review, vigilance, misuse/off-label monitoring…).
Is the CEP/CDP mandatory for legacy devices under MDR?
Yes. All devices, including legacy ones, must have a Clinical Evaluation Plan (CEP) and Clinical Development Plan (CDP) under the MDR framework.
How should manufacturers handle update frequency of the CER in terms of Quality Management System (QMS)?
The QMS should have a Clinical Evaluation procedure (SOP) compliant with MDR requirements and include the update frequency according to the classification and implantable status.
Should the SSCP readability test for the patient section be performed at each update?
Yes. It is recommended to include the readability test (Flesch-Kincaid is commonly used) in a QMS procedure to ensure its application at each update of the patient section.
Can manufacturers use MEDDEV 2.7/1 Rev. 4 under the MDR?
Yes, selectively. While the MDR supersedes MEDDEV guidance, some parts—especially related to CER methodology and update frequency for Class I devices—remain referenced (e.g., section 6.2.3). However, MDR-specific articles must prevail in case of conflict.
Can manufacturers harmonize the update cycles for CER, PSUR, PMCF, and SSCP?
Yes, and it is strongly recommended to harmonize these processes within your QMS by generating a documented device cycle with set timelines for the various activities as described in the example in this blog. One of the goals of the MDR’s evidence loop is to ensure temporal alignment between these documents. Harmonized cycles prevent inconsistencies and support a synchronized narrative across technical documentation. It also demonstrates that the post-market surveillance system is effectively integrated into the manufacturer’s QMS and lifecycle management.
What are the risks if one document is updated but the others are not?
Misalignment between documents, such as an updated PSUR without corresponding updates in the CER or SSCP, can be flagged as a nonconformity during an audit. Notified Bodies expect consistency across clinical evidence outputs. If new clinical or safety data are not reflected in all relevant documents, this could indicate a fragmented or reactive clinical evaluation process. Maintaining a tracking log of interlinked updates is the best practice.
